

Abstract
Introduction: Chronic transfusion is a therapeutic modality in the prevention and treatment of end-organ damage in sickle cell disease (SCD) patients. Central venous access devices (CVAD) are commonly used in many SCD patients due to poor venous access. However, CVAD is a known risk factor for venous thromboembolism (VTE) (Evans et al, 2010), with right atrial thrombi prevalence estimated between 5.4 and 12.5% (Shah et al., 2004; Gilon et al., 1998). Although SCD is a prothrombotic state (Wun et al, 2013), it is not known whether this risk factor interacts with CVADs in a synergistic manner to increase the overall risk of VTE. No study has specifically addressed the role of thromboprophylaxis for CVAD-related VTEs in SCD, and as such the practice of prophylactic anticoagulation and/or antiplatelet therapy for CVAD is heterogeneous. We therefore conducted a quality improvement study to investigate whether thromboprophylaxis is a protective factor for new catheter-related thrombi (CRT).
Methods: By cross-referencing imaging, thrombosis clinic, and sickle cell clinic databases, we identified adult SCD patients (≥ 18) of all genotypes followed within the Toronto General Hospital SCD center between January 1, 2009 and December 31, 2017 who had a CVAD intended for long-term use (≥3 months). CRT was defined as a VTE that developed while the CVAD was in place. Patients with no VTE during CVAD placement were assigned to the comparator group. Patients who were on anticoagulation for any alternative reason prior to CVAD insertion were excluded. The presence, type, and intensity of pharmacological thromboprophylaxis at the time of CRT or line insertion were recorded. Patient, catheter, and treatment-related risk factors of VTE were extracted from electronic patient records. Fisher-exact and chi-square tests were conducted to explore possible associations between categorical co-variates, and thromboprophylaxis use. Linear regression was performed for continuous variables; while binary logistic regression was conducted to examine the potential association between thromboprophylaxis use and CRT, while adjusting for sex, genotype, hydroxyurea use, and concomitant thrombosis risk factors.
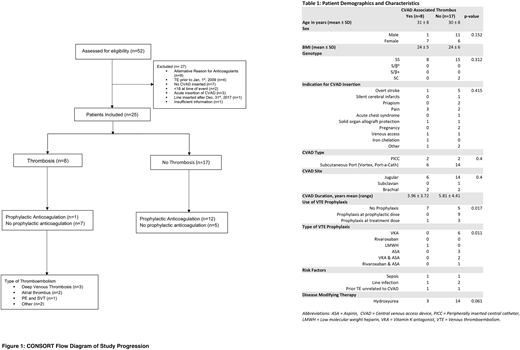
Results: We identified 52 unique patients from 3 databases. After applying the inclusion and exclusion criteria, 25 patients were retained as stated in Figure 1-CONSORT Flow Diagram. Patient characteristics are summarized in Table 1-Patient Demographics and Characteristics. Events were distributed as follows: 3 deep venous thrombi, 1 superficial venous thrombus, 1 pulmonary emboli, 2 right atrial thrombi, and 2 thrombi from other sites. Patients with CRT incurred significant sequelae, including open heart surgery to remove the clot in the two patients with right atrial thrombi. Univariate analysis illustrated association between the development of a CRT and the use of thromboprophylaxis, type of thromboprophylaxis, and dose intensity (p=0.011, p=0.011 and p=0.017, respectively). HU use showed a trend towards lower risk for CRT (OR 0.129, p=0.061). However, CRT was not associated with gender, genotype, type, site of insertion, year of insertion, duration of insertion, indication for CVAD, BMI, or ferritin. Association between CVAD thromboprophylaxis and CRT remained significant despite adjusting for sex, genotype, HU and concomitant thrombosis risk factors in binary logistic regression (p=0.032). Patients who received pharmacologic thromboprophylaxis for CVAD were 30.9 times less likely to have a CRT. Due to the limited sample size, not all variables could be included in the logistic regression.
Conclusion: The presence of a CVAD is a significant risk factor for VTE in SCD patients. The retrospective study demonstrated that CRTs are associated with the absence of pharmacological thromboprophylaxis for CVADs. In addition, the potential role of HU in reducing thromboembolic risk in SCD patients with CVADs, requires further exploration. Finally, in the event that a CVAD is unavoidable we recommend consideration of pharmacologic thromboprophylaxis, in order to reduce patient morbidity and health-care associated costs.
Forté:Novartis: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal